Analysis of the socket bone wall dimensions
Analysis of the socket bone wall dimensions
The success of dental implantation is, in large part, contingent on our understanding of the healing process of the hard and soft tissues surrounding the implant site. Knowledge of the healing process, which is constantly increasing, also contributes to the manufacturing of better implants with improved surface qualities and designs.
One of the ways to minimize the number of surgical procedures, for the benefit of the patient and the clinician, is to place the implants in the extraction sockets immediately after the tooth is removed; however, this is not always possible because the anatomy of the tooth and root often do not match that of the implant, so the lack of congruence of the socket and the implant may complicate the surgical procedure. The reabsorption of the tissues, which commonly occurs under these circumstances, can also hamper the healing process. Due to these potential complications, this method of immediate implantation is regarded as a highly advanced procedure.
The clear advantage of immediate implantation is the preservation of the architecture of the bone surrounding the socket; however, the soft and hard tissues surrounding the extraction site, from both the buccal (cheek) and lingual (tongue) sides, undergo reabsorption without the support of the extracted tooth. This process cannot be avoided by immediate implantation,
and therefore much caution is needed when this procedure is selected.
Studies suggest that the width of the buccal bone may have a significant effect on the reabsorption process. Most studies agree that a minimum of 2 mm of bone is required to avoid bone loss and encourage both faster healing and a better aesthetic outcome; if this requirement is not met, a procedure of ridge augmentation is most commonly performed.
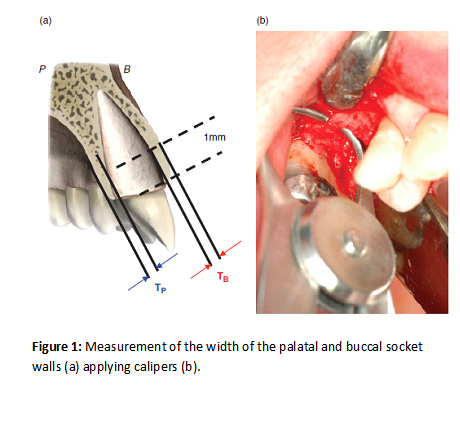
In a study conducted by Huynh-Ba et. al (“Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement” published in “Clinical oral implants research”, 2009) the socket dimensions of 93 patients, candidates for immediate implantation, were measured as shown in Figure 1.
The mean values of the width of the buccal and palatal (lingual) bony walls of the socket are presented in Figure 2.
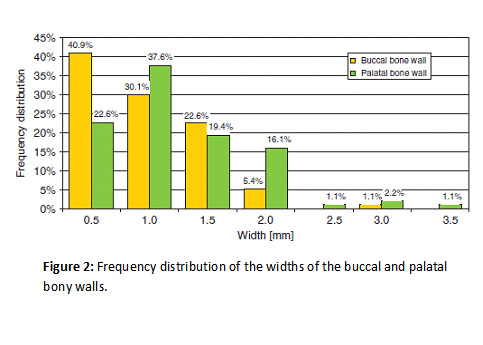
The results show that the mean width of the buccal and palatal bony walls of these 93 extractions sites was 1 mm and 1.2 mm, respectively. Only 6.5% of the patients had a buccal bone that fit the recommendations for immediate implantation – 2 mm width. 79.5 of the patients had palatal bony wall less than 2 mm wide.
Considering the common recommendation nowadays, that immediate implantation should be performed only when the bony walls of the extraction socket are 2 mm or more, these results suggest that this recommendation is not necessarily met in the majority of the cases. This may damage the healing process and inhibit successful implantation. As the authors mark, in such cases where the width of the bony walls of the socket are less than 2 mm, auxiliary procedures, such as guided bone regeneration and ridge augmentation, may be required to achieve successful healing and better aesthetic results.
* Adapted from: Huynh-Ba G, Pjetursson BE, Sanz M, Cecchinato D, Ferrus J, Lindhe J, Lang NP. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin. Oral Impl. Res. 21, 2010; 37–42.